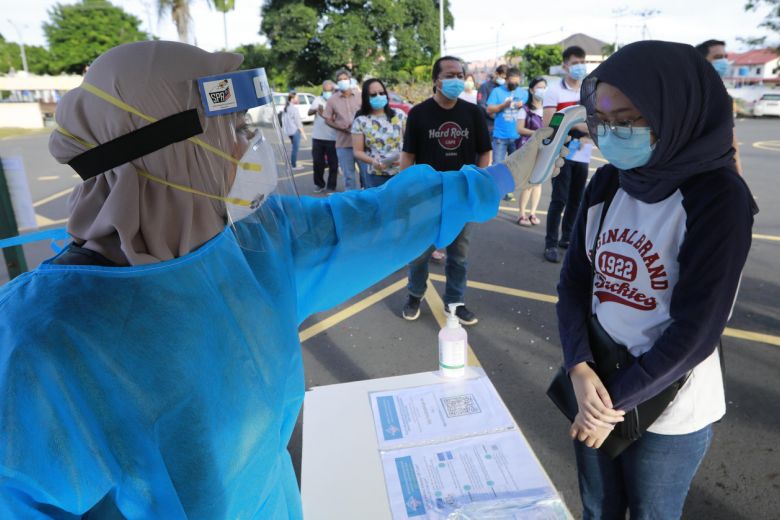
As Malaysia is facing another surge of Covid-19 cases, it is imperative that the government is well prepared to handle the crises and does not face a similar situation as India. In the midst of all this, it is very important to focus on the rural communities. The situation of healthcare in rural parts of the country seems to be shaky and needs serious policy interventions from state, federal government, and other important stakeholders.

Lack of Access To Healthcare Facilities
One of the main issues is that there is a lack of access to healthcare facilities. For comparison, 92% of Malaysia’s urban population live within 3 kilometres of a clinic or hospital, whereas only 69% of the rural population live near a healthcare centre[7]. For healthcare to be accessible and equitable it is paramount rural communities get the same quality and care they need, when they most need it.

Lack of Infrastructure
The Ministry of Health (MOH) needs more funding to fill the gap in infrastructure[7]. Rural hospitals need investment in technology so that there is no need to travel to cities.Inclusion of technology greatly helps to improve the quality of healthcare. Rural areas also require more hospitals. By ensuring more hospitals people would get quality healthcare at their footsteps. The lack of infrastructure prevents people from accessing healthcare facilities. The states of Sarawak and Sarawak terrains are so rugged that it is very difficult to have proper infrastructure built[2].

Lack of Medical Equipment
Current medical facilities just provide basic services, so for complex medical procedures people have to travel to town centres for treatment. It has been reported that 70.7 % of Sarawak hospitals do not provide laboratory services. Although there are alternatives provided by the MOH such as Flying Doctor Service (FDS) it has a limited impact. FDS only goes to villages and other rural parts only once a month[1]

Lack of Professional Medical Personnel
Although the urban population has more requirements, after analysing the data, it can be concluded that the number of medical professionals available is still distributed disproportionally. Sarawak and Sabah, the two rural states in East Malaysia face acute shortage of medical professionals. This can be proven easily after analysing the doctor to patient ratio. For example in Sarawak, there was only one doctor for every 682 people[1]. This is 1.5 times less than the nationwide ratio. There is no doubt that there are vast inequalities among the urban and rural parts of Malaysia. Hospitals in rural Malaysia are being run by nurses and medical assistants. This has a direct impact on the quality and quantity of medical service in rural parts.

Challenge in attracting quality human resource to rural states
The lack of proper infrastructure acts as a huge barrier of encouraging young doctors to provide their services in rural parts of the country. Deployment of qualified medical personnel remains unpopular. For doctors, these postings are often unrewarding and come with no benefits[3]. The same issue was also raised by Deputy Health Minister Aaron Ago Dagang , who is also an MP from Sarawak. During his interaction, he reiterated the fact that most of the doctors after training do not get jobs due to the fact that they are not willing to move to rural areas. In a 2010 study evidence shows that doctors are not willing to give up luxuries of city life[3]. There needs to be concentrated efforts by the government and various stakeholders to encourage medical professionals to shift to rural parts. One possible solution to this is to provide extra financial support as recommended by the Malaysian Medical Association. They argue that there needs to be a structural deployment planning with incentives such as re-deployment in urban areas after certain years of service in rural areas[3].
Voice of the voiceless
On ground there are various people who are playing a very critical and important role in bringing these issues into light. Agnes Padan, a Sarawakian rural health activist who has fought for the need of specialists in Sarawak’s hospitals[4]. She was also recently appointed PKR Sarawak Women chief. Her whole activism has been structured around raising voices for inequalities present in the health ecosystem. Her activism also focuses on breast cancer screening of Sarawak women. She has continuously highlighted the difficulties of women in the state to undergo a test for breast cancer.
Government’s Action Plan
To overcome these lack and challenges, the government has provided several of the following initiatives[6]
- Payment of Insentif Wilayah (District Incentive) at the rate of 12.5 to 25 % of the monthly salary.
- Payment of Insentif Pedalaman (Interior Incentive) for officers at Sarawak at a rate of 10% of monthly salary.
- Payment of Insentif Penempatan Pakar Perubatan (Medical Specialist Placement Incentive)
In Sarawak, the MOH is planning to hire at least 100 permanent and 50 contract officers to fill the gap this year .
Most of the rural health care is provided by public health care facilities as the private sector are not able to make profits due to low income population. In order to cover a population that is unable to obtain treatment from public facilities, 1Malaysia Clinics were established in 2009[11]. The clinics are managed and run by Assistant Medical Officers (AMC). There are more than 3,000 clinics, which caters to 95% of the population[5].
Another promising change in Malaysia is the rise of telemedicine. Telemedicine refers to a patient being treated remotely, where the doctor is located in another city. Recent studies have shown that there is a general acceptance among patients and doctors but unfortunately many rural areas do not have electricity let alone internet[7]. To overcome this, the MOH needs to work with different stakeholders to solve connectivity issues.
Covid-19 vaccine and logistics:
Certain Covid-19 vaccines require very sophisticated protocols to store them, which rural regions lack. Malaysia plans to achieve herd immunity by the end of this year[8], but for this to happen it is very important there is a structural mechanism to distribute vaccines to rural areas. Rural areas face major challenges in vaccinating its population. In Sarawak, 75 remote clinics are only accessible by river. The lack of infrastructure means that they are mostly difficult to access hence, a different approach needs to be done for rural folks[1]. To address this problem it was decided by the government that rural communities will receive Astrazeneca vaccines as they require normal temperature storage.
Providing rural communities with Pfizer vaccines is a very costly business. It is estimated that the cost of each freezer is RM 80,000 and based on that, it would cost RM 3.6 million alone to provide cold storages in Sabah and Sarawak hospitals alone[10]. The other concern that is being raised is that in the National Immunisation Programme (NIP), a very low number of Vaccines Administered Centres (VACs) allocated in states such as Kelantan, Johor, Sabah and Sarawak.

Covid-19 has taught us that governments all around the world should invest in healthcare and build a sustainable health system that is structured around the welfare of the people. For Malaysia, there needs to be a proper framework and plan which tackles the issues in rural areas and finds sustainable solutions. For Malaysia to become a high income country it is foremost to lessen the gap of healthcare facilities between urban and rural communities.
Explore Our Sources:
- Batumalai, K (2020). 57 Years Later, Do Sarawak, Sabah Enjoy Equal Health Care To Peninsula? [online]. Kuala Lumpur: Code Blue. Link
- Wiki Impact (2020) Four Clear Reasons Why Healthcare In Rural Malaysia Needs Attention [online]. Link
- Ibrahim, Mohamed Izham Mohamed, et al. “Evaluation of Knowledge and Perception of Malaysian Health Professionals about Telemedicine.” Journal of Clinical and Diagnostic Research Vol. 4, No. 1, 2010, pp. 2052–56. Link
- Chiam, A (2020). Rural health activist Agnes Padan appointed as PKR S’walk Women chief [online]. Kuching: Borneo Post. Link
- Koshy, Rachel, KM Noh, K Juval, K Agamutu, and M Nazimin Shamsuddin. “Flying Doctor Service in East Malaysia.” European Journal of Public Health. Vol. 23, No. 1, 2013. Link
- CodeBlue (2020) Sarawak Has 1.5 Times Fewer Doctors Per Population Than Nationwide Malaysia [online]. Link
- Falcon,D. (2019) The Health Care Gap in Rural Malaysia.Perspectives on Business and Economics Volume 37. Link
- Free Malaysia Today (2021) Herd immunity unlikely until next year, unless it is redefined, says MP [online]. Link
- Batumalai,K (2021) Last Mile Covid Vaccine Delivery Far From Perfect in Sabah, Sarawak. Code Blue 12th January, 2021 [online]. Link
- Yeo, A (2021) Vaccination Challenges In Rural Sabah & Sarawak [online].Kuala Lumpur: Emir Research. Link
- Mahadeva, Sanjiv, Hematram Yadav, Simon M Everett, and Khean-Lee Goh. “Economic Impact of Dyspepsia in Rural and Urban Malaysia: A Population-Based Study Journal of Neurogastroenterology and Motility Vol. 18, No. 1, 2012, pp. 43–57. Link
Written by: Suhaib Shaukat

